
HIPAA Authorization Form Template Word

The HIPAA Authorization Form Template Word is a comprehensive and customizable document that helps healthcare providers comply with the Health Insurance Portability and Accountability Act (HIPAA) regulations. This template is designed to be used by medical professionals who need to obtain written authorization from patients before disclosing their protected health information (PHI) to third parties.
The HIPAA Authorization Form Template Word is easy to use and can be customized to meet the specific needs of your practice. The template includes all the necessary elements required by HIPAA, such as the patient’s name, date of birth, and contact information, as well as a description of the PHI that will be disclosed and the purpose of the disclosure.
Using this template can help you save time and ensure that you are in compliance with HIPAA regulations. It can also help you protect your patients’ privacy and avoid potential legal issues. The HIPAA Authorization Form Template Word is available for immediate download and can be used on any computer with Microsoft Word installed.
Key features of the HIPAA Authorization Form Template Word include:
- Customizable fields for patient information and PHI disclosure
- Clear and concise language that is easy for patients to understand
- Compliance with all HIPAA regulations
- Immediate download and use on any computer with Microsoft Word
Overall, the HIPAA Authorization Form Template Word is an essential tool for any healthcare provider who needs to obtain written authorization from patients before disclosing their PHI to third parties. It is easy to use, customizable, and compliant with all HIPAA regulations, making it a valuable addition to any medical practice.
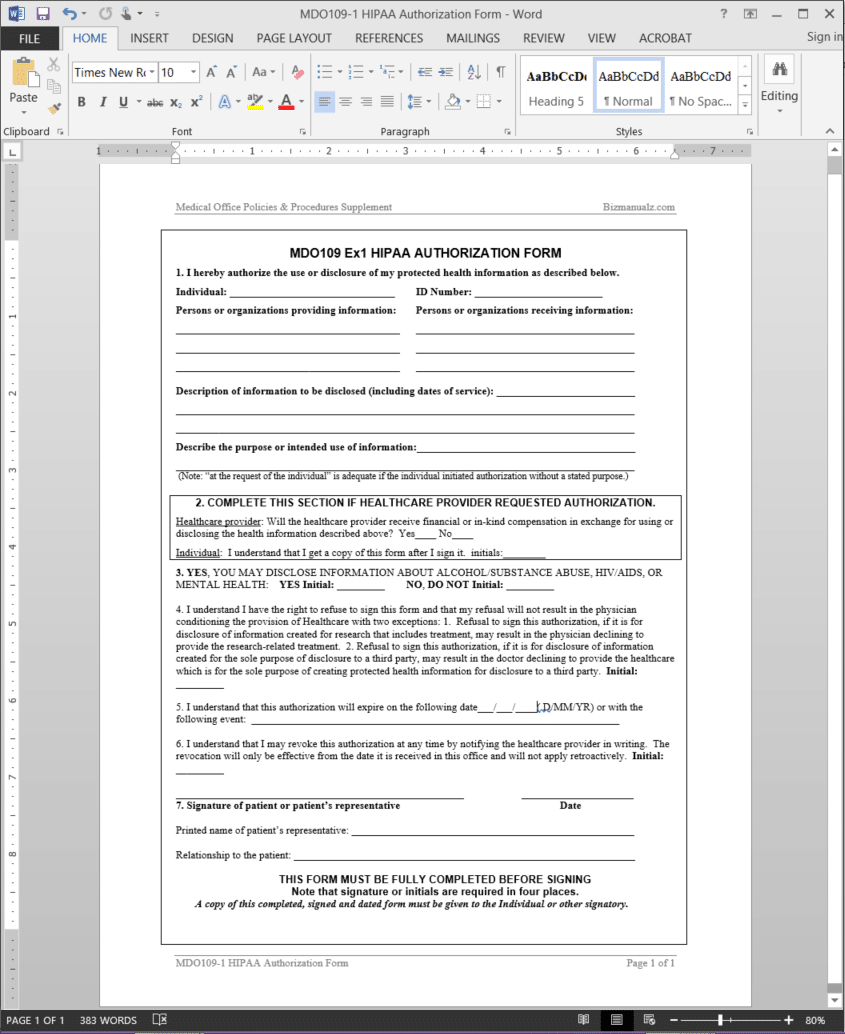
>HIPAA Authorization Form Template
The HIPAA Authorization Form Template authorizes the use or disclosure of protected health information. By signing this form, the individual understands that he/she may revoke authorization at any time by notifying the healthcare provider in writing. The revocation will only be effective from the date it is received in the office and will not apply retroactively. MDO109-1 HIPAA AUTHORIZATION FORM and the information requested should be kept in each record.
The Office Manager should adopt a written privacy procedure that clearly identifies employees or classes of employees who require access to protected information, how it will be used within the entity, and when the information may be disclosed. To protect patient privacy, employees must take extra precautions, both in structures and in circumstances, not to inadvertently release patient information. Patients may choose to deny the provider from using their information for a variety of reasons. Patients can opt out of any portion of the notice.
 HIPAA Authorization Form Template Details
HIPAA Authorization Form Template Details
Pages: 01
Words: 383
Format: Microsoft Word 2013 (.docx)
Language: English
Manual: Medical Office
Procedure: Health Insurance Portability Accountability Procedure MDO109
Type: Form

Reviews
There are no reviews yet.